
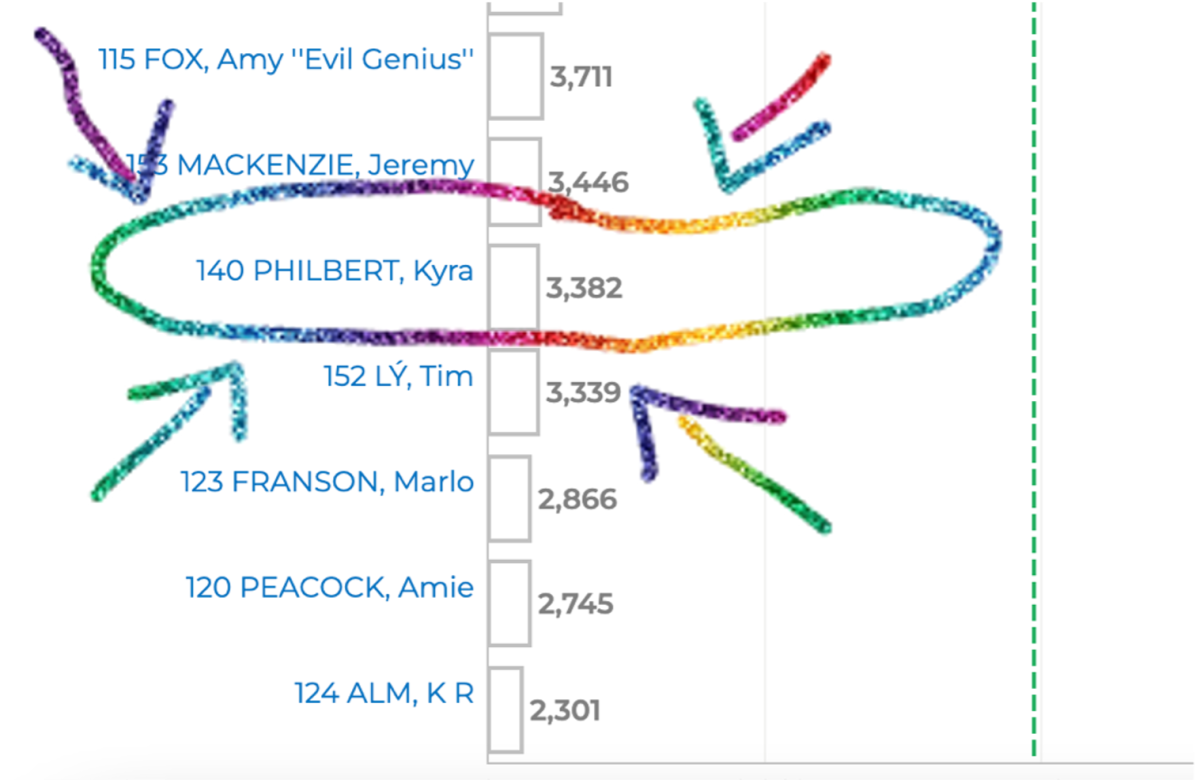
Well, the results are in! I did not get elected for ‘Vancouver’ City Council during the October 15th, 2022 municipal elections. Unlike most of Vancouver’s Reddit community, I don’t need to imagine getting less votes than Amy “Evil Genius” Fox nor Rollergirl. With a resounding 3 382 votes, I’ve lived it, and I can use my creative thinking for other things. Also, it was super exciting. I absolutely thought I would get 50 votes max. If you voted for me: wow! thank you! endless gratitude for supporting my vision for radical, intersectional, queer, feminist, compassionate healing…Considering that I did no active campaigning, made no promotional materials, talked to no strangers (dangers), put up a few social media videos to my 300 then followers, got zero media coverage and did one debate (thanks Vancouver Public Space Network!)… I feel proud of my first foray into politics!
I’m not even remotely upset about my defeat… I am way too focused on that a ton of people voted to increase the police everywhere: schools, parks, every city block?
Excuse me while I go vomit.
I am in anger and disgust now. Honestly- I spent Saturday night, and nearly all day Sunday and Monday just bawling my eyes out. Sad about our new reality in a police state. Sad about the scary drought/fires/smoke. Sad because I was not expecting this result (naïve much?). Sad that I feel so betrayed by fellow citizens. How dare you! All these folks claim to be concerned about the DTES and helping people… so like my job for the last six years… ? They are concerned about Chinatown and helping the seniors out… so again, my job for the last six years…? They claim they want nurses providing an empathic response… so again, my literal job for the last six years. They claim they want solutions… but what outcome are they looking for?
***
To add insult to injury, the major elect, Ken Sim, and his party are trying to make nurses complicit in their pro-police agenda- particularly mental health nurses. Today, on CBC radio, he stated “to give your listeners a little bit about my background […] my background is in nursing… so we understand the moving parts” [11:03-11:09] – I am not a journalist, but I can tell you, he is not registered with the college. Being an employer of nurses is not the same as having a “background in nursing”. As a self-governed profession, ‘nurse’ is a protected title. He did not say, “I’m a nurse” but he certainly implied he had an expertise in nursing that that he may or may not hold. Nurses are a highly respected and trusted profession in Canada. He is falsely leading the public into a belief that trusted professionals, like nurses, think more police is a good idea. In actuality, many Canadian nurses are calling for the complete abolition of both the police and prison systems.

Can an actual journalist investigate Ken Sim’s claim about his ‘background in nursing’ and if it is misleading to people ? Can you also ask the BCCNM if it violates the use of the reserved nursing title?
I mean, maybe I am wrong and Ken Sim does have a real background in nursing. In which case, I want to know: where did Ken Sim get his nursing degree? Who is Ken Sim’s favourite nursing theorist? What is his area of clinical expertise? Where has he practiced?
Until then, if you want to hear Stephen Quinn interview an *actual* nurse, you can listen my interview with him from May.
*********
Nursing, like policing, is a problematic institution. It is based in white ideology, it has a history based on anti-Blackness, and that context has had very direct harms for folks of colour. Nursing, like policing, are composed of individuals – some are very lovely people (and some are murderous assholes)! However we work in *systems* and those systems make us do things that are straight up racist like birth alerts! Or arrest people because they peed outside! I am including myself in this.
Here’s a scenario : a young brown person is brought to the emergency room by the police. They are there to have their dog bite wounds treated, sustained during their arrest. Their crime was shoplifting (total amount, under 20$) and then fleeing. The police dog was deployed to apprehend the suspect/victim. The person was bitten on multiple points of their body, notably their head. Police dog should be trained to release their bite on command. The patient was bitten by the dog on their head/face repeatedly. The extent of the damage is deeply disturbing: They will require extensive plastic surgery, their vision will be forever impaired and they will have an obvious lifelong facial disfigurement. Worse, their healing outcomes are poor: the nurse expects that the person will develop infections and require repeated rounds of IV antibiotics due to the nature of the trauma [dog bite], and the conditions of the patient’s lifestyle (poverty, insecure housing, malnutrition). Each probable infection represents the possibility of a preventable death from sepsis. The police are joking in the trauma bay and minimising the harms the patient will now have to live with for their rest of their life. They do not reconsider their actions until the nurse informs them how much money this dog bite will cost our public medical system… their empathy is with the tax payer, not the real human whose life they have forever fucked. The patient is discharged back into police custody. The nurse is very distressed, and wants to take action. They are actively discouraged by hospital leadership from calling in a complaint to the VDP about the behaviour of the police re: excessive force. The nurse is reminded that VPD is a community partner. The nurse does not feel safe nor supported by the larger medical system. The nurse does not feel like they are acting within their own moral framework, nor their professional ethics. Still, the nurse does not report. They go home, cry in the shower and try to scrub off the shame/guilt/disgust.
****
It’s not a personal insult to be critical of the systems we engage with, particularly if they are harming people. I am certain lots of people went into policing because they wanted to make a positive impact in their community! However, structures of power need to be actively unlearned. Nurses have an ethical obligation towards social justice. Nursing is very actively trying to address its racism problem. My own scholarship does this– no one bats an eye when I tell them that nursing is racist… it is a fact! A necessary fact to openly acknowledge to shift the profession towards anti-racism.
Meanwhile, while I was calling the police complaint line during the ‘freedom convoy’ in Vancouver [which happened while our CAPITAL was OCCUPIED! Hello, it was fricking domestic terrorism! just need to go vomit again] – and I stated a fact: the police are a system build on racism. I was told not to be ‘controversial!’.
AHHHHHH
AHHHHHH
AHHHHHH
The complaint officer kept interrupting me, and comparing his experience as a white man going abroad to my own ! He demanded that I listen to him, while he spoke soooooooo slowly about *his* feelings of becoming cognisant of his race for like 2 seconds in a temporary position of his own making as the benevolent Canadian on voluntourism!… he said this to me while I was actively fearful for my safety within my own city [on unceded territories of the Sḵwx̱wú7mesh, Səl̓ílwətaʔ/Selilwitulh and xʷməθkʷəy̓əm Nations] .
He said this to me while I was getting ready to march back and forth at Main & Kingsway holding a little dinky sign in an effort to delay traffic slightly.
He said this to me while I spent the day bawling because I was so scared. My co-protesters were trying to be positive, with music and fun outfits. They were trying to cheer me up because I was very miserable and clearly alone… but (a) stranger danger (b) I did not want to have to mask my feelings for the comfort of randos when it was a very scary/upsetting situation, (c) I think crying was an appropriate response to what was going on!

PHOTO BY JEFF VINNICK /PNG
He said this to me while his colleagues would yell at me to hurry up. “Ma’am! I’m worried about your safety!”. I would think that I know how to cross a goddamn fucking street! and they don’t care about *my* safety because if they did I would be sipping tea at home, not actively witnessing people honking their cars [and drive in from the burbs while unnecessarily emitting fossil fuels!], trying to block access to the major hospital, yelling transphobic stuff and doing white power gestures.
AHHHHHHHH
Eventually I said to the complaint officer, “I’m pretty sure your job is just to listen to my concern and log it… and I want you to do that now”. Judging from that interaction, it is clear to me that there has been very little critical thinking within the VPD about their social responsibility towards dismantling the systems of inequity. The focus is repeatedly on ‘public safety’– well safety for who? from what?
I am so sad and scared, yet again.
*****
The mayor elect Ken Sim’s rationale for mental health nurses working with the police is there would be a more ’empathic’ response. He claims he wants to be evidence-based. So let’s explore that claim – that nurses working with police generate more empathic responses- with a recently published academic article about mental health, policing and nursing in a British Columbian context. The lead author of the article, Maja Kolar (they/them) is a registered psychiatric nurse, holds a master of science in nursing, and very cool.
Kolar et al. (2022) employed critical discourse analysis to examine the provincial legislation The Metal Health Act (1996) and its interpretive handbook, the Guide to the Mental Health Act (2005). The act directs the involuntary and voluntary psychiatric treatment for folks in British Columbia experiencing mental health issues. Nurses, physicians, and police officers are professionals who regularly enact the act, which gives them authority to intervene on someone experiencing mental health issues. Kolar et al. identified “the need for protection” as a central discourse within these texts. The authors affirm the term protection is never clearly defined within the act but rather, the word’s use is broad. This lack of clarity around what constitutes protection allows the safeguard of the enforcers while legitimizing involuntary psychiatric treatment.
The police are given power via Section 28: Police Intervention for public safety to bring someone experiencing mental distress in for a medical examination in a hospital setting. This form of policing is considered an enforcement of protection through containment. Kolar et al. comment that this type of policing reinforces both the criminalization and stigmatization of folks experiencing mental health issues. They also highlight the danger of police intervention which “increases the likelihood of involuntary treatment, as well as detention, incarceration, violence, and in extreme circumstances, death of people experiencing mental health and/or substance use issues”(Boyd and Kerr, 2016; Wilson-Bates, 2008 as cited by Kolar et al., 2022, p. 11). Regarding my own profession, nurses might make clinical assessments on recalling a patient on extended leave based on missed medication or appointments. Together, a nurse and police officer might work together to locate a patient “for apprehension and transport to hospital” (Kolar et al., 2022, p. 11). Kolar et al. are mindful that neither the act nor the guide pays attention to nursing practice. The result is an invisiblization of how nurses might be complicit as agents of enforcement, within these structures of power that actively harm. Not to mention nurses acting in ways that go against our professional ethical obligations and best practice: harm reduction/ trauma informed. My own experience validates this concern.
Ken Sim’s claim that the nurse might provide a more empathic response is not supported by this evidence. The empathic and compassionate response I would want to provide to patients is made impossible by the presence of police. Perhaps he is conflating the presence of the nurse with less lethal outcomes for folks… but that does not mean it is a ‘good’ solution. Kolar et al. actually recommend intervening on social conditions like poverty, racism, unsafe housing, transphobia, and colonialism. What if we actually did stuff to prevent the need for a mental health crisis response in the first place?
****
There is a cycle:
without equity action to address the social determinants of health
a person’s mental state deteriorates
so badly
that eventually
they fit the criteria
to be removed
contained
detained
for ‘public safety’
by police
[and nurses]
and sometimes police + nurses working together.
***
I could not find any academic research about Car 87/88. This is the program that Ken Sim wants to expand by hiring all these mental health nurses. However, I can share from my experience working in a major emergency department in Vancouver that Car 87/88 were mostly bringing people in from their extended leaves [recalling]. My interactions with the teams were positive, and I think they do an important service for loved ones wanting to assist someone in crisis and de-escalating that situation.
However, the larger conversation that dominated the election was about ‘public safety’, crime and the DTES. Ken Sim stated in his CBC interview that increasing Car 87/88 alone would not be enough. “We need to go upstream, we need to figure out what the root causes of these challenges are and it could be… mental health, addictions, people experiencing homelessness…” [0803-0813]. Okay, well, that’s easy enough because it’s poverty.
****
For a long time, Vancouver’s DTES has been a containment zone. According to Dana Culhane (2003, p. 594) “Public health and law enforcement authorities, in an effort to respond to these “twin epidemics” [Kyra note: HIV + IV drug use] have treated the Downtown Eastside as a containment zone, rather than as an enforcement zone: few if any arrests are made for simple possession or trafficking of small quantities of illegal drugs, or for soliciting for the purposes of prostitution.” Now in 2022, we have even more epidemics to add: Covid 19, opioid poisoning crisis, missing & murdered women… [which is still happening, vomit, like the circumstances of Chelsea Poorman’s death that the VPD ruled not suspicious].

Yet where is the DTES? It is obvious to me that this area is a heterotopia. The city has historically used this space to contain all its undesirables. The DTES is simultaneously Chinatown [headtax], Japantown [internment], Hogan’s Alley [destruction for the viaduct] and Strathcona [for ethnic Europeans like Italians, until they got absorbed into white]…

The new mayor will have a “satellite city hall in Chinatown”. The Chinatown Business Association is focused on the promotion of Chinatown with their first item being (1) security patrol [aka, protect settler capital] and then (2) cleaning graffiti [aka beautification]. Their website make no mention about the other places/spaces that encompass Chinatown (for example: DTES/Hogan’s Alley). It focuses on tourism, profit, and revitalisation… which means
the undesirables
the trash
[the poverty]
must be contained… elsewhere.
****
The police might be up for the job… but I really hope nurses take a clear stand against this. This work goes against all evidence and our professional values. There is nothing that suggests nurses are ‘more’ empathetic to these situations other than that they get forced into being complicit and maybe make it less likely the police will immediately kill someone. There is no rationale that the police could not get training to be more empathic themselves (and clearly they desperately need it!).
The evidence for the root cause of these problems is overwhelming. The evidence against doubling down on policing is also overwhelming. Yet Ken Sim wants us… so as nurses, we have the power of the powerless here. All nurses can take a radical stand and refuse to do this outrageous work. Instead, that money can be reallocated into actually addressing the social determinants of health with radical interventions of care: finding safe & secure housing for people, feeding people and ending poverty.
I hope that we are supported by our nursing leadership at multiple levels: our major union [BCNU], our professional associations [CNA, NNPBC], our major employers [like the health authorities: VCH, PHSA, Providence], our college [BCCMN] and all our nursing scholars/researchers in the lower mainland. It would be very impactful if all these groups– who have made pretty significant claims of anti-racism and equity– now enacted their politics! Statements/press conferences/ big stink. The use of nurses for pro-police rhetoric must be challenged.
***
There is certainly a way for Chinatown to be fabulous, and everyone to have a cute time… but it’s not achieved through policing! The police only deal with a situation, after it has already happened. We got to invest in prevention and intersectional equity. It’s great that the new mayor has endorsed all the equity policy asks from women transforming cities’ hot pink paper campaign, among them washrooms for all, healing lodge, and alternative non-police models to community safety. These were also election promises, that will make an actual difference. I want to see how Ken Sim follows up on those.
but what do I know… I’m a loserrrrrrrrrrr
***
(if you liked this post, you might like “Kyra Philbert is impotent” — a post I wrote in the immediate aftermath of the first major sweep along the 00-100 blocks of Hastings in the Spring of 2023)
